- Visibility 185 Views
- Downloads 18 Downloads
- DOI 10.18231/j.ijce.2021.014
-
CrossMark

Stamp technique to restore occlusal anatomy of the posterior tooth: A case report
Introduction
Nowadays, doing composite restoration is new norm because of increase concern for esthetics. The rapid increase in composite resin restoration is also due to the introduction of minimally invasive restorative procedures that emphasize the maintenance of healthy tooth structure and the use of adhesive material in the posterior region.[1]
However, the composite still has some drawbacks. Its multiple procedures take time and require excellent dexterity and skill of the operators to achieve a harmonious occlusion and cusp fossa relationship with opposing teeth. The time required to complete the restoration is double compared to amalgam.[2]
So, A technique was proposed by Dr. Waseem Riaz a London based practitioner which is a known as ‘Stamp technique’ in which direct composite resin restorations was used to obtain the precise occlusal topography easily. It has also been reported for vertical bite reconstruction of worn out dentitions.[3]
This new technique consists of making an occlusal index which records the posterior teeth occlusal anatomy prior to cavity preparation.[4], [5] The index thus obtained is then pressed against the final composite increment before curing to obtain a positive replica of the preoperative anatomy. The only scenario in which stamp technique is therefore feasible is when the tooth being operated upon has intact anatomical features. This implies that occult caries with clinically imperceptible cavitation can be restored by the stamp technique.[6]
Here we reported two cases where we used stamp technique for management of class I (pit and fissure) caries in posterior teeth.
Case 1
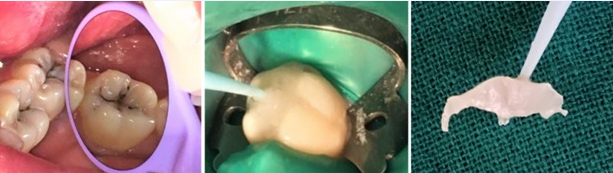
19-year female patient presented with complain of food lodgment in lower left back tooth region since 1 month. On clinical examination, pit and fissure caries were detected in relation to 36. The marginal ridges were intact and there was no significant cavitation. The tooth was isolated with a rubber dam and a separating agent was brushed onto the tooth area. A flowable composite resin (Ivoclar Tetric N-Flow) was applied to the intact occlusal surface and indexed on cusp tips. A microbrush tip was cut off and the microbrush was used as a handle. The handle was immersed in the composite before being cured by LED light to make the occlusal stamp. All the caries was removed and class I cavity was prepared. Etching was done using 37% phosphoric acid (Ivoclar N Etchant Gel). Bonding agent (Ivoclar Tetric N-Bond) was applied and cured for 20 seconds with LED curing light. After this cavity has been restored using composite resin (Ivoclar Tetric N Ceram) gradually leaving 1 mm of the occlusal surface. After application of the last layer of composite resin, Teflon tape was been placed on the occlusal surface. The stamp was placed on the tape and then the composite resin was polymerized. Finishing and polishing was done using composite finishing and polishing kit.

Case 2
A 21-year-old woman reported blackish discoloration of tooth in lower right back region. During the examination, a class I cavity was visualized on tooth 47. After oral prophylaxis and isolation with rubber dam, a small amount of flowable composite material (Filtek flow, 3M ESPE, St Paul, MN, USA) was placed on the occlusal surface of the affected tooth. The tip of the applicator brush was then immersed in this composite and the composite was then cured. Following this, the cavity preparation was carried out. Etching was done using 37% phosphoric acid (3M ESPE Scotchbond Universal Etchant). Bonding agent (3M ESPE Adper Single Bond2) was applied and the composite resin was placed in increments and polymerized for 20 seconds by LED curing light. After the application of the last layer of composite resin, a Teflon tape was placed on the occlusal surface. The stamp was laid on the tape, then the composite resin (3M Filtek Supreme) was cured with LED curing light for 20 sec. The finishing and polishing were performed using a finishing and polishing kit.


Discussion
Restoring the actual topography of the tooth surfaces will certainly promote patient’s compliance and acceptance of dental treatment. This case report describes a simple technique to obtain a good surface finish and occlusal anatomy of the direct posterior composite with minimal time using the stamp technique with flowable composite.
Trauma from occlusion is an iatrogenic wound if it is not taken into account during the operative procedure would modify the stability of the entire stomatognathic system.[7] A functional occlusion promotes a favorable adaptation of the neuro-musculature, the temporomandibular joint, teeth and its supporting structures while maintaining a positive and stable inter-cusp relationship in centric occlusion without symptoms of mandibular dysfunction and without signs of tooth wear.[8], [9] The importance of occlusion is paramount because orofacial integrity is the key element for psychosocial well being.
The stamp technique procedures are very simple and achievable for Class I cavities. The flowable composite can be applied on the occlusal surface directly without the need of isolation agent. However, if deep pits and fissures are present on tooth, use of the isolation agent is recommended. In such condition, the isolative material fills the pits and fissures and does not allow the subsequent flowable composite to flux inside. This leads to continuous surface of the final restoration. Thus, use of extreme air spray should be avoided while spreading the isolation agent on the tooth surface.[4]
The major advantage of this technique is reduced overall time due to almost instantly desired good cusp–fossa relationship and there is reduction of porosity in final restoration along with decrease in the formation of microbubbles and interference of oxygen during polymerization of composite as the stamp matrix exerts pressure on composite.
Stamp technique is suitable technique in a busy practice to dealing with many patients, as minimal time is required for finishing to obtain a good fossa-cusp relationship with the opposing dentition.[4]
The disadvantages of the technique includes breakage of stamp, and cost of flowable composite.
Initially, time utilized for mastering the technique is more but, this can be easily overcome with practice. With correct and precise placement of stamp accurate cusp fossa relation can be obtained.
Conclusions
The stamp technique is a procedure which is easy to follow and can efficiently recreate the occlusal anatomy resulting in a biomimetic restoration. It can be used effectively when the occlusal anatomy is not much distorted.
Source of Funding
No financial support was received for the work within this manuscript.
Conflict of Interests
The author declares that they do not have any conflict of interests.
References
- CA Murdoch-Kinch, ME McLean. Minimally invasive dentistry. J Am Dent Assoc 2003. [Google Scholar] [Crossref]
- D C Dilley, W F Vann, T R Oldenburg, R M Crisp. Time required for placement of composite versus amalgam restorations. ASDC J Dent Child 1990. [Google Scholar]
- ST Ramseyer, C Helbling, A Lussi, Lussi. Vertical Bite Reconstructions of Erosively Worn Dentitions and the “Stamp Technique” - A Case Series with a Mean Observation Time of 40 Months. J Adhesive Dent 2015. [Google Scholar]
- S A Alshehadat, MS Halim, K Carmen, CS Fung. The stamp technique for direct Class II composite restorations: A case series. J Conserv Dent 2016. [Google Scholar] [Crossref]
- Thomas Attin, Florian J. Wegehaupt. Impact of erosive conditions on tooth-colored restorative materials. Dent Mater 2014. [Google Scholar] [Crossref]
- JGF Pompeu, R C Morais, T O Ferreira. Occlusal Stamp Technique For Direct Resin Composite Restoration: A Clinical Case Report. Int J Recent Sci Res 2016. [Google Scholar]
- E P Dawson. Evaluation, Diagnosis and treatment of Occlusal problems. 2nd Edn. . [Google Scholar]
- T M Roberson, I V Heymann, H V Swift, J Edward, M Clifford. Sturdevant’s Art and Science of Operative Dentistry. 5th Edn. 2006. [Google Scholar]
- I Klienburg, R Jagger. Occlusion and Clinical Practice: An Evidence Based Approach. 1st Edn. 2004. [Google Scholar]