- Visibility 48 Views
- Downloads 2 Downloads
- DOI 10.18231/j.ijce.2021.023
-
CrossMark

Comparative evaluation of shaping ability of trunatomy and protaper gold files in curved canals using cone?beam computed tomography: An invitro study
Introduction
Cleaning and shaping of the root canal is a crucial procedure in endodontic treatment that influences the subsequent steps in the procedure.[1] As it is an important aspect, researchers and manufacturers are in a constant race to attain the perfect alloy and instrument design for minimally invasive preparation and preservation of the remaining dentin thickness.[2] The continuous research in the field of Nickel-titanium (NiTi) rotary instruments to enhance their cutting and shaping characteristics have proved that these instruments create more centered preparation of the canal, with less transportation compared to stainless steel instruments. [3] The evolvement in the field of NiTi rotary instrument to optimize their characteristics have introduced many new systems into the market, due to which dental practitioners need an equitable evaluation of these systems to guide them select one of the best systems available. [3]
Recently TruNatomy (TN; Dentsply Sirona, Maillefer, Ballaigues, Switzerland) NiTi rotary system was introduced. This file system is manufactured from a 0.8mm NiTi wire instead of 1.2mm NiTi wire that is used to manufacture most generic files and exibits off-centred parallelogram cross section. It is a system with advanced engineering to offer the benefits like improved performance and efficacy, preservation of structural dentin, and maintain the strength of the tooth by respecting the tooth anatomy.[4] TruNatomy files contain a TN orifice modifier (tip size 20 with a taper of 0.08), TN Glider (tip size 17 with taper of 0.02) to obtain a glide path. the shaping files are available in different sizes and lengths to treat different cases. It consists of TN Prime shaping file (tip size 26 with a taper of 0.04) which is suitable for most cases. Two additional shaping files, TN Small (tip size 20 with taper of 0.04) for smaller canals amd TN Medium (tip size 36 with taper of 0.03) for larger canals.
ProTaper Gold (PG) (PG; Dentsply, Tulsa Dental Specialties, Tulsa, OK, USA) is another NiTi rotary system developed with exclusive advanced metallurgy. It features a progressively tapered design that claimed to improve the cutting efficiency and safety. PG system has been metallurgically enhanced through heat treatment and exhibits a convex triangular cross‑section. [1] PG files are available in eight sizes: SX (tip size 19 with a taper of 0.04), S1 (tip size 18 with a taper of 0.02), S2 (tip size 20 with a taper of 0.04), F1 (tip size 20 with a taper of 0.07), F2 (tip size 25 with a taper of 0.08), F3 (tip size 30 with a taper of 0.09), F4 (tip size 40 with a taper of 0.06), and F5 (tip size 50 with a taper of 0.05). [5]
This study intends to compare the canal transportation and canal centering ability in the preparation of curved root canals after instrumentation with TruNatomy and ProTaper Gold files using cone‑beam computed tomography (CBCT).
Materials and Methods
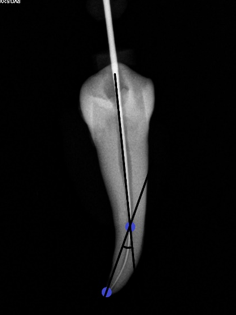
30 single rooted extracted human teeth for reasons unrelated to this study were selected. The sample size was estimated based on previous litreture and derived using a scientific formula. Teeth were accessed using an Endo‑Access bur (Dentsply Maillefer) in a high‑speed handpiece. Canal patency was obtained by inserting size 10 K‑files (Dentsply Maillefer) through the canals, and the canal curvature was evaluated according to Schneider’s method ([Figure 1]). [6] Only canals with curvatures of 20−30° were included in this study.
Teeth with any visible cracks or fractures, calcifications, previous root canal treatments were excluded. Each sample was allotted a number from 1 to 30. Working length was determined by apex locator (Dentaport- Root Zx, J Morita). The teeth were randomly assigned into two groups i.e. Group 1-TN (TruNatomy) and Group 2-PG (Protapter Gold) (n = 15 each).
Root canal shaping
Canals were instrumented by a single operator according to the manufacturer’s instructions for both the systems. An electric motor (X-smart, Dentsply Sirona) was used to operate the files. Stainless steel #15 K-file was used to establish glide path upto predetermined working length. In both groups, after each file, the canals were irrigated with 2 mL of 2.5% sodium hypochlorite. A lubricant Glyde (Dentsply Maillefer) was used during instrumentation. All instruments were used for the preparation of only 3 canals. Group 1-TN root canal were intrumented using the TN orifice modifier, TN Glider followed by TN Prime shaping file. The sequence in which root canals in group 2-PG were instrumented was: SX, S1, S2, F1, and F2. All instruments were used for the preparation of only 3 canals.
Image analysis
The roots were placed in a custom‑made specimen holder in which each root was positioned in the same place before and after instrumentation. The roots were aligned perpendicularly to the beam and were scanned before and after instrumentation using the CBCT scanner. The roots were scanned before and after instrumentation using the CBCT scanner (Kavo OP 3D Pro, Germany) operating at 90kV, 8 mA. The field of view was 8x8 cm. Slices were 800 × 800 pixels, with a pixel size of 0.125 mm.
Cone‑beam computed tomography measurements
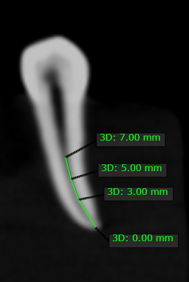
Pre‑ and post‑instrumentation measurements of canals were achieved using the On-demand 3D CBCT software. Canal transportation and centering ratio was calculated at three cross‑section levels, i.e., 3, 5, and 7 mm ([Figure 2]) from the apical end of the root using the following equation.
Degree of canal transportation = (X1−X2) − (Y1−Y2)
Canal centering ratio = (X1−X2) / (Y1−Y2) if (X1−X2) < (X1−X2) or
(X1−X2) / (Y1−Y2) if (Y1−Y2) < (X1−X2)
Where,
X1 is the shortest distance from the mesial edge of the root to the mesial edge of the uninstrumented canal,
X2 is the shortest distance from the mesial edge of the root to the mesial edge of the instrumented canal,
Y1 is the shortest distance from the distal edge of the root to the distal edge of the uninstrumented canal, and
Y2 is the shortest distance from the distal edge of the root to the distal edge of the instrumented canal
Statistical analysis
The data analysis was done using SPSS software and the test used was independent sample t test for comparison between the 2 groups.
Results
The mean and standard deviation values for canal transportation and centering ability at the 3 different levels for both the groups, are displayed in table 1 and table 2 respectively. Looking at the apical portion of the root canal i.e. 3mm, there is no significant difference for canal transportation in both the groups. At 5mm the comparison between two groups showed statistically significant difference for canal transportation (p=0.01). At 7mm the comparison showed no significant difference between both groups for canal transportation.
A highly statistical significant difference of P=0.008 was found for canal centering ability at the apical portion when the two groups were compared (P<0.5) at. The results after comparison between two groups at 5mm and 7mm for canal centering ability were not statistically significant.
|
Canal Transportation |
Group |
Mean |
Std. Deviation |
t |
Significance |
|
3mm |
Protaper Gold |
0.07 |
0.07 |
0.229 |
0.82 |
|
TruNatomy |
0.07 |
0.06 |
0.229 |
||
|
5mm |
Protaper Gold |
0.11 |
0.07 |
2.759 |
0.01* |
|
TruNatomy |
0.05 |
0.05 |
2.759 |
||
|
7mm |
Protaper Gold |
0.07 |
0.07 |
-0.07 |
0.944 |
|
TruNatomy |
0.07 |
0.08 |
-0.07 |
|
Canal Centering |
Group |
Mean |
Std. Deviation |
t |
Significance |
|
3mm |
Protaper Gold |
0.70 |
0.29 |
2.843 |
0.008* |
|
|
TruNatomy |
0.43 |
0.25 |
2.843 |
|
|
5mm |
Protaper Gold |
0.55 |
0.17 |
-0.822 |
0.418 |
|
|
TruNatomy |
0.62 |
0.29 |
-0.822 |
|
|
7mm |
Protaper Gold |
0.63 |
0.33 |
1.71 |
0.098 |
|
|
TruNatomy |
0.40 |
0.39 |
1.71 |
|
Discussion
Canal transportation is defined by glossary of endodontic terms as: Removal of canal wall structure on the outside curve in the apical half of the canal due to the tendency of files to restore themselves to their original linear shape during canal preparation; may lead to ledge formation and possible perforation. [7] Centering ratio is a measure of the ability of the instrument to stay centered in the canal. Smaller the ratio, the better the instrument will remain centered in the canal. [8]
In this study canal transportation was determined by the formula developed by Gambill et al. : (X1 - X2) - (Y1 - Y2). [8], [9] Where, X1 is the shortest distance from the outside of the canal to the periphery of the uninstrumented canal. Y1 is the shortest distance from the inside of the root to the periphery of the uninstrumented canal. X2 is the shortest distance from the outside of the root to the periphery of the instrumented canal. Y2 is the shortest distance from the inside of the root to the periphery of the instrumented canal. If the result obtained from this calculation using the above-mentioned formula is 0, indicated that there is no canal transportation.
Centering ratio was also calculated by the formula developed by Gambill et al.: (X1 - X2)/(Y1 - Y2). [8], [9] Where, if (X1 - X2) and (Y1 - Y2) were not equal, then the lower figure was considered as the numerator of the ratio and a result of one obtained from the formula indicated perfect canal centering by the instrument used.
This study compared the canal transportation and centering ability of two different NiTi rotary systems i.e. TruNatomy (TN; Dentsply Sirona, Maillefer, Ballaigues, Switzerland) and ProTaper Gold (PG) (PG; Dentsply, Tulsa Dental Specialties, Tulsa, OK, USA). TruNatomy (TN; Dentsply Sirona, Maillefer, Ballaigues, Switzerland) NiTi rotary system was manufactured from a 0.8mm NiTi wire instead of 1.2mm NiTi wire that is used to manufacture most generic files and exibits off-centred parallelogram cross section. It is a system with advanced engineering to offer the benefits like improved performance and efficacy, preservation of structural dentin, and maintain the strength of the tooth by respecting the tooth anatomy. [4] TruNatomy files contain a TN orifice modifier, TN Glider with shaping files available in different sizes and lengths to treat different cases. It consists of TN Prime shaping file which is suitable for most cases. Two additional shaping files, TN Small for smaller canals amd TN Medium for larger canals.
ProTaper Gold (PG) (PG; Dentsply, Tulsa Dental Specialties, Tulsa, OK, USA) is another NiTi rotary system developed with exclusive advanced metallurgy. It features a progressively tapered design that claimed to improve the cutting efficiency and safety. PG system has been metallurgically enhanced through heat treatment and exhibits a convex triangular cross‑section. [1] PG files are available in eight sizes: SX, S1, S2, F1, F2, F3, F4, and F5. [5]
This study aimed to compare the canal transportation and canal centering ability in the preparation of curved root canals after instrumentation with TruNatomy and ProTaper Gold files using cone‑beam computed tomography (CBCT).
Canal transportation and centering ability was determined at three levels which included the measurements 3, 5, and 7 mm, form the root apex that represented the apical, middle, and coronal thirds of the root canals. The angle of curvature of the root canals choosen was 20–30° and is considered as moderate curvature according to American Association of Endodontists (AAE) Endodontic Case Difficulty.
The results of canal transportation and centering ratio revealed that there were significant differences between TN and PG systems in canal transportation at 5mm from the apex and centering ratio at 3mm from the apex. TN system showed comparatively less canal transportation at the middle third of the root canal when compared with PG system. Where as, PG system showed better centering ability at apical third of the root canal when compared to newly introduced TN system. The maximum value of root canal transportation in tested groups was lower than the shortest distances from the outside of the curved root to the periphery of the uninstrumented canal. Overall, no systems exceeded the 0.3-mm limit for transportation that is considered critical for the clinical prognosis at any level. Hence, both the used systems can be considered suitable for the preparation of the curved root canals. [10]
A study compared shaping ability of WaveOne Gold (WG; Dentsply Tulsa Dental Specialties, Tulsa, OK), the Reciproc Blue (RB; VDW, Munich, Germany), TRUShape (TS, Dentsply Tulsa Dental Specialties), XP-endo Shaper (XP; FKG, La Chaux-de-Fonds, Switzerland), iRace (IR, FKG), and TruNatomy (TN; Dentsply Sirona, Ballaigues, Switzerland) for preparation of moderately curved canals which used micro–computed tomographic technology. This study concluded that TN and XP preserved the canal anatomy, but TN touched the lowest percentage of canal surface (50%). [11] This may affect the biomechanical preparation of the root canal as all the canal surfaces are not touched by the file. But on the other hand a case report published concluded that the TN system preserved original canal anatomy, dentine thickness and maintained the structural integrity of teeth which is an integral part of root canal shaping and preparation. The case report also stated that focusing on the benefits like dentine preservation, improved performance and efficacy the TruNatomy instruments offer the clinician superior debridement by respecting original canal anatomy. [12] Another study where double curverd simulated canals were used concluded that TN files maintained the original canal shape and also prepared canals more efficiently and removed less resin, and PG which had largest apical taper showed more transportation in the apical curvature area when compared to other niti files systems. [13]
Conclusion
Within the limitations of this study, TN resulted in less transportation than PG at the middle third, and PG showed better centering ability at the apical third. but the clinical importance of these differences can be considered limited. Overall, both systems safely prepared root canals, causing minimal errors. Future research should be focused on comparing TN system in moderately and severely curved canals and comparing their ability to preserve the root canal anatomy and canal shaping efficiency with systems manufactured from similar metallurgy.
Conflict of Interest
The authors declare that there are no conflicts of interest in this paper.
Source of Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- AM Elnaghy, SE Elsaka. Shaping ability of ProTaper Gold and ProTaper Universal files by using cone-beam computed tomography. Indian J Dent Res 2016. [Google Scholar] [Crossref]
- MLN Perez Morales, JAG Sánchez, JGO Fernández, K Laperre, FA Sans, DE Jaramillo. TRUShape versus XP-endo Shaper: A micro-computed tomographic assessment and comparative study of the shaping ability-An in vitro study. J Endod 2020. [Google Scholar] [Crossref]
- J Gagliardi, MA Versiani, MD Sousa-Neto, A Plazas-Garzon, B Basrani. Evaluation of the shaping characteristics of ProTaper Gold, ProTaper NEXT, and ProTaper Universal in curved canals. J Endod 2015. [Google Scholar] [Crossref]
- AM Riyahi, A Bashiri, K Alshahrani, S Alshahrani, HM Alamri, D Al-Sudani. Cyclic Fatigue Comparison of TruNatomy, Twisted File, and ProTaper Next Rotary Systems. Int J Dent 2020. [Google Scholar] [Crossref]
- D Tulsa. The ProTaper Gold Brochure. 2014. [Google Scholar]
- SW Schneider. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971. [Google Scholar]
- . American Association of Endodontists. Glossary of endodontic terms. American Association of Endodontists. 2003. [Google Scholar]
- H Selvakumar, V Anandhan, E Thomas, K Swaminathan, R Vijayakumar. Evaluation of canal transportation and centering ability of K3(0.02%) and K3(0.04%) with hand K files in primary teeth using spiral computed tomography. J Indian Soc Pedodontics Prev Dent 2014. [Google Scholar] [Crossref]
- JM Gambill, M Alder, CE del Rio. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod 1996. [Google Scholar] [Crossref]
- M Wu, B Fan, P Wesselink. Leakage Along Apical Root Fillings in Curved Root Canals. Part I: Effects of Apical Transportation on Seal of Root Fillings. J Endod 2000. [Google Scholar] [Crossref]
- MlN Pérez Morales, JAG Sánchez, JG Olivieri, F Elmsmari, P Salmon, DE Jaramillo. Micro–computed Tomographic Assessment and Comparative Study of the Shaping Ability of 6 Nickel-Titanium Files: An In Vitro Study. J Endod 2021. [Google Scholar] [Crossref]
- PJ Van Der Vyver, M Vorster, OA Peters. Minimally invasive endodontics using a new single-file rotary system. Int Dent-Afr 2019. [Google Scholar]
- H Kim, S J Jeon, M S Seo. Comparison of the Shaping Ability of ProTaper GOLD, WaveOne GOLD, and TruNatomy in Simulated Double-curved Canals. . [Google Scholar] [Crossref]