- Visibility 30 Views
- Downloads 3 Downloads
- DOI 10.18231/j.ijce.2021.027
-
CrossMark

Endodontic management of Type-2 and Type-3 C-shaped root canal system in mandibular second molars: A case series
Introduction
An essential pre-requisite for the success of endodontic treatment is a thorough knowledge of root canal anatomy and its variations. The prognosis of endodontically treated tooth largely depends on the meticulous cleaning, shaping and filling of the complex root canal system.[1] A large variation in canal configuration is seen among teeth; mandibular second molar being of particular interest. Cooke and Cox in 1979 [2] was first to document C-shaped canal in literature. It is commonly observed in mandibular second molar, can also be seen in mandibular premolars [3] and maxillary first molars. [4] The cause of formation of C-shaped canal is the failure of fusion of hertwig’s epithelial root sheath. Conical/prism shaped root are formed because of failure of fusion of hertwig’s epithelial root sheath on both buccal and lingual side. [5] This configuration shows ethnic predilection showing high prevalence among Asians. [6], [7]
It is found up to frequencies to 52% in chinese population, and maximum frequencies of 2.7–10.6% in other populations. [8], [9] In some case reports and studies variation-shaped canals in maxillary first molars, mandibular first molars, mandibular premolars and third molar teeth had been reported. [10], [11] For a C-shaped root canal, both anatomic and radiographic classifications have been proposed. C-shaped root canal configuration can vary along the root length is common factor of all classifications. [12] Present case series reports two different cases of C-shaped root canal system in mandibular second molar.
Case Report 1
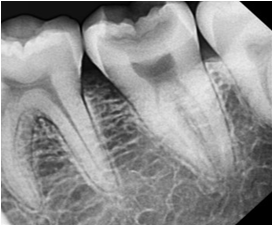
A 43 years old male patient reported in the Department of Conservative Dentistry and Endodontics with chief complaint of pain in the lower left tooth back region since past 5 days. Patient also reported sensitivity due to hot and cold food which got subsided on removal of the stimuli. No relavant medical history was reported. On clinical investigation, deep occlusal cavitated lesion with positive tender on percussion was present in mandibular left second molar (#37). Radiographically, caries was seen extending till pulp in relation to tooth #37. This case was diagnosed as irreversible pulpitis in relation to tooth #37. ([Figure 1])
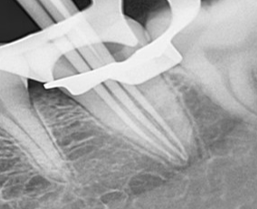
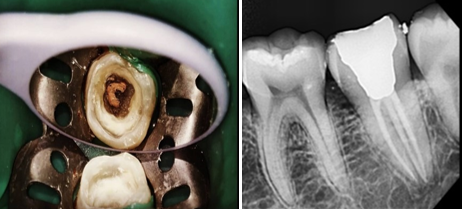
Under profound anaesthesia and in under rubber dam isolation, access cavity was prepared. Working length was estimated radiographically with 10nos K-File in three canals. ([Figure 2]) In tooth #37, three orifices were located and prepared till F1 size of Protaper Universal file system (Dentsply Maillefer, Ballaigues, Switzerland). Radiograpically, corresponding F1 size gutta percha cones was selected as master cone fit. ([Figure 3]). All the three canals were filled with gutta percha and sealer using cold lateral condensation technique. The endodontic cavity was restored back with a flowable bulk fill composite resin. ([Figure 4]).

Case Report 2
36 years old female patient reported complaining of pain on mastication in the lower right back tooth region. Medical history of the patient was not significant. On clinical examination, deep occlusal carious lesion approaching pulp was seen in mandibular right second molar (#47). Pulp vitality test shows that tooth was non vital and was tender on percussion. On radiographic examination, there was a presence of periapical radiolucency with tooth #47. An diagnosis of acute periapical abscess was made in tooth #47. It also showed a single conical root with three radiolucent canal outline, which were joining at the apical third of the root, which suggest C-shaped canal pattern is present.
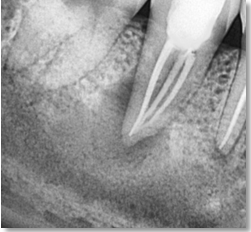
An access cavity was prepared after proper isolation and profound anesthesia. Three orifices were recognized on exploration of pulp chamber, which were then negotiated with the use of multiple small K-files (8,10,15 nos). During working length determination, radiograph shows that all the canals were joined at the apical third of the root.([Figure 5]) ProTaper rotary files (Dentsply Maillefer, Ballaigues, Switzerland) were used for cleaning and shaping of the canals till the size F2. An intracanal medicament, calcium hydroxide (RC-Cal, India) was administered and the patient was recalled after one week. In the next appointment, intracanal medicament was removed followed by copious irrigation with normal saline and 3% NaOCl. Master cone snug fit was checked radiographically([Figure 6]), and the canals were obturated with single cone technique.([Figure 7])


Discussion
A unique root canal configuration, mostly found in mandibular second molars is a C-shaped canal configuration with a prevalence that ranges between 2.7%–52% in different populations. Based on anatomic and radiographic appearance, a few classifications of C-shaped canals have been published. It has been seen that C-shaped canal systems have many variations such as single and ribbon-like canals from orifice to apex, distinct root canals or fins or webs connecting the individual root canals. Therefore, C-shaped canals are known to present a complex canal anatomy.[12] Melton et al. derived a classification based on the cross-sectional shape of the canal viz; continuous C shaped (C1), semicolon (C2) and separate canals (C3).[13] As per this classification, our first case reported here in the paper is C3 type and second case report is C2 type. In most cases danger zone is present, which is the mesiolingual area of dentine surrounding the canal which is thinner than the other side of the root and hence, C-shaped canals are not centralized.[14]
Hand and rotary files are used for traditional cleaning and shaping of C-shaped canals. More or less round-shaped canal cross-sections are formed as a result of use of both types of instruments, however they leave up to 66% of the canal wall uninstrumented.[15], [16] Hence, the additional use of tissue dissolving irrigants and intracanal dressings is necessary. Only agents used in endodontics that display some tissue-dissolving ability are sodium hypochlorite.[17], [18]
Along with conventional therapy the use of ultrasonics would be more effective. Deeper penetration with small instruments using sonics or ultrasonics and an increased volume of irrigant may allow for more cleansibility in fan-shaped areas of the C-shaped canal.[19]
Gulabivala et al.[20] reported the incidence of 22.4% in Burmese patients using a canal staining and tooth clearing technique. In another study he noted the prevalence of 10% in Thai population using the injection of Indian ink,[21] while high incidence of C-shaped canal system (41.27%) in mandibular second molars of a Chinese population is found by Wang et al.[22]
Conclusion
For successful endodontic therapy, knowledge of different possible alterations in the internal anatomy of teeth is important. Difficulties in debridement, filling, and restoration occur due to C-shaped canal system and considerable variation in their anatomical configuration. However a combination of proper diagnosis, proper technique of cleaning, debridement and obturation is necessary for this kind of root canal anatomy and for attaining success in these cases.
Conflict of Interest
The authors declare that there are no conflicts of interest in this paper.
Source of Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- G Jain, K Agarwal, PS Samant, V Srivastava. Demystifying anatomical variations – Endodontic therapy of twin rooted mandibular canine with concomitant root canals: An unusual case report. IP Indian J Conserv Endod 2020. [Google Scholar] [Crossref]
- H Jafarzadeh, YN Wu. The C-shaped Root Canal Configuration: A Review. J Endod 2007. [Google Scholar] [Crossref]
- N Velmurugan, R Sandhya. Root canal morphology of mandibular first premolars in an Indian population: a laboratory study. Int Endod J 2009. [Google Scholar] [Crossref]
- S Sidow, LA West, FR Liewehr, R Loushine. Root Canal Morphology of Human Maxillary and Mandibular Third Molars. J Endod 2000. [Google Scholar] [Crossref]
- SA Manning. Root canal anatomy of mandibular second molars.. Int Endod J 1990. [Google Scholar] [Crossref]
- Z P Yang, S F Yang, Y C Lin, J C Shay, C Y Chi. C-shaped root canals in mandibular second molars in a Chinese population. Endod Dent Traumatol 1988. [Google Scholar]
- MS Seo, DS Park. C-shaped root canals of mandibular second molars in a Korean population: clinical observation andin vitroanalysis. Int Endod J 2004. [Google Scholar] [Crossref]
- Y Wang, J Guo, H B Yang, X Han, Y Yu. Incidence of C-shaped root canal systems in mandibular second molars in the native Chinese population by analysis of clinical methods. Int J Oral Sci 2012. [Google Scholar]
- R T Walker. Root form and canal anatomy of mandibular second molars in a southern Chinese population. J Endod 1988. [Google Scholar]
- BM Cleghorn, WH Christie, CCS Dong. Anomalous mandibular premolars: a mandibular first premolar with three roots and a mandibular second premolar with a C-shaped canal system. Int Endod J 2008. [Google Scholar] [Crossref]
- D Keinan, E Nuni, I Slutzky-Goldberg. Is a C-shaped configuration possible in teeth other than mandibular molars?. Quintessence Int 2009. [Google Scholar]
- DC Melton, KV Krell, MW Fuller. Anatomical and histological features of C-shaped canals in mandibular second molars. J Endod 1991. [Google Scholar] [Crossref]
- H Jafarzadeh, YN Wu. The C-shaped Root Canal Configuration: A Review. J Endod 2007. [Google Scholar] [Crossref]
- W Chai, YL Thong. Cross-sectional Morphology and Minimum Canal Wall Widths in C-shaped Roots of Mandibular Molars. J Endod 2004. [Google Scholar] [Crossref]
- F Paqué, D Ganahl, OA Peters. Effects of Root Canal Preparation on Apical Geometry Assessed by Micro–Computed Tomography. J Endod 2009. [Google Scholar] [Crossref]
- M Solomonov, F Paqué, B Fan, Y Eilat, LH Berman. The Challenge of C-shaped Canal Systems: A Comparative Study of the Self-Adjusting File and ProTaper. J Endod 2012. [Google Scholar] [Crossref]
- G Hasselgren, B Olsson, M Cvek. Effects of calcium hydroxide and sodium hypochlorite on the dissolution of necrotic porcine muscle tissue. J Endod 1988. [Google Scholar]
- M Andersen, A Lund, JO Andreasen, FM Andreasen. In vitro solubility of human pulp tissue in calcium hydroxide and sodium hypochlorite. Dent Traumatol 1992. [Google Scholar] [Crossref]
- DC Melton, KV Krell, MW Fuller. Anatomical and histological features of C-shaped canals in mandibular second molars. J Endod 1991. [Google Scholar] [Crossref]
- K Gulabivala, TH Aung, A Alavi, YL Ng. Root and canal morphology of Burmese mandibular molars. Int Endod J 2001. [Google Scholar] [Crossref]
- K Gulabivala, A Opasanon, YL Ng, A Alavi. Root and canal morphology of Thai mandibular molars. Int Endod J 2002. [Google Scholar] [Crossref]
- Y Wang, J Guo, H B Yang, X Han, Y Yu. Incidence of C-shaped root canal systems in mandibular second molars in the native Chinese population by analysis of clinical methods. Int J Oral Sci 2012. [Google Scholar]