- Visibility 58 Views
- Downloads 13 Downloads
- DOI 10.18231/j.ijce.2021.036
-
CrossMark

Endodontic management of multiple roots and root canals in mandibular canine: A case report series
Introduction
The aim of the root canal treatment is the complete elimination of infection from the root canal and the prevention of reinfection.[1]
The major issues that occur during the endodontic treatment are due to the insufficient knowledge of the anatomy of the root canal space.[2] The main reason for failure of the root canal treatment is that the inability to obturate one of the root canal because of ignoring the variations of the both internal and external anatomy of the involved tooth.[3] An extensive knowledge of the normal and variations in anatomy of teeth is important to make sure the success of a root canal treatment.[4] Mandibular canines normally have single root and single canal is 87%. In 10% of cases, there are two canals join at the root apex and in 3% have completely separated two canals.[5] Conventional radiographs may not give details about the root canal configuration in teeth with complex root canal morphology such as multiple root canals and extra roots, especially when present in buccolingual direction. Inadequate details may lead to poor prognosis. Advanced radiographic techniques such as the cone‑beam computed tomography (CBCT) may result in three‑ dimensional evaluation of root canal configuration, thus predicting success.[6] This article presents two case reports with respect to the endodontic management of mandibular canines with single root and two root canals.[4]
Case Report
Case 1
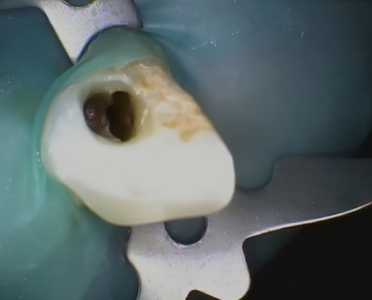
A 30-year-old men reported to the department of Conservative dentistry and Endodontics with the chief complaint of pain in lower left front tooth region. On examination, left lower canine was secondary carious and nonresponsive to electric pulp tester [[Figure 2]].
A diagnosis of secondary caries involving pulp was made in response to 33 and treatment plan was made as root canal therapy followed by crown. Tooth was isolated using rubber dam.
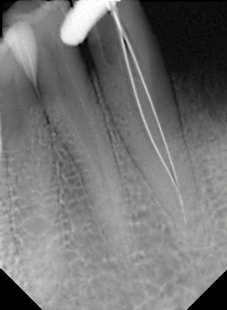

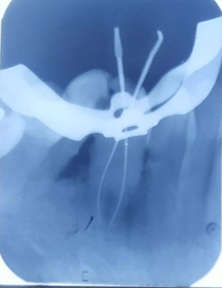
The secondary caries was removed and the canine access was made from the lingual aspect. The lingual and buccal orifices were identified and negotiated with no 10 k files. The GG drill no 1, 2 were used in crown down method to enlarge the orifices and to have the straight line access into the canal. The working length was measured with the help of an apex locator as 19mm in both the buccal and lingual canal and verified with radiograph [[Figure 3]].
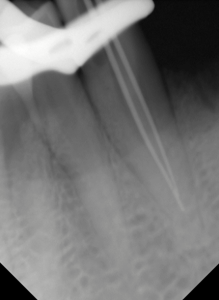
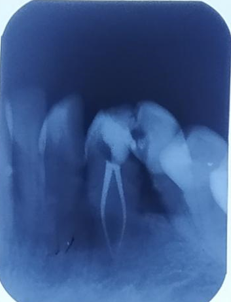
Coronal flaring was carried out using the Sx file of the ProTaper system (Dentsply, Maillefer, Ballaigues, Switzerland). Individual canal flaring was performed with ProTaper (Dentsply, Ballaigues, Switzerland) rotary NiTi files. During instrumentation, irrigation was performed with 2.5% sodium hypochlorite. All canals were prepared to a size F2 file. After completion of the biomechanical preparation, root canals were dried with paper points and then obturated with Gutta percha. AH plus was used as a sealer. A post- operative radiograph was taken ([Figure 5]) which showed a satisfactory obturation. After one week, the patient was asymptomatic and a final composite restoration was performed.[[Figure 4], [Figure 5]]
Case 2
A 35-year old female patient was reported to the Department of Conservative Dentistry & Endodontics suffering from severe pain in her lower right anterior region. The chief complaint of the patient was “Sharp intermittent pain upon both hot and cold stimulus, sometimes the pain was continuous and awakened her at night”.
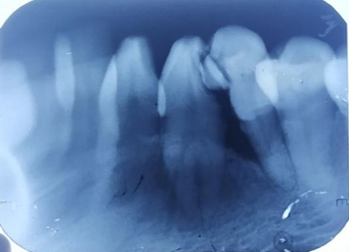

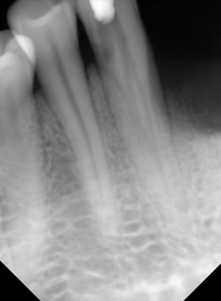
Clinical examination revealed a mandibular right canine with extensive proximal caries and tender to percussion. Vitality tests on the involved teeth showed abnormal responses (lingering pain to cold, increased reaction at Electrical Pulp Test). Pre-operative radiographs revealed deep proximal caries encroaching the pulp with two roots and two root canals ([Figure 6]). The diagnosis of irreversible pulpitis was made for the right mandibular canine and nonsurgical root canal treatment was scheduled for the involved tooth.
After the administration of the local anesthesia and under rubber dam isolation, caries was removed and the pulp chamber was accessed. To gain sufficient access to the canals, the conventional lingual access opening was modified into one that included more the incisal surface. On entry into the pulp chamber, two main orifices were found: one lingually and one buccally. Coronal flaring was carried out using the Sx file of the ProTaper system (Dentsply, Ballaigues, Switzerland). The two canals were identified and negotiated with a size 10 K-file. The working length of the located canals was established with the use of an apex locator as 18mm in both buccal and lingual root and verified by taking a radiograph ([Figure 7]). Individual canal flaring was performed with ProTaper (Dentsply, Ballaigues, Switzerland) rotary NiTi files. During instrumentation, irrigation was performed with 2.5% sodium hypochlorite. All canals were prepared to a size F2 file. After completion of the biomechanical preparation, root canals were dried with sterile paper points and then obturated using Gutta percha. AH plus was used as a sealer. A post- operative radiograph was taken ([Figure 9]) which showed a satisfactory obturation. After one week, the patient was asymptomatic and a final composite restoration was performed.
Discussion
Proper diagnosis and careful clinical and radiographic inspection, the Endodontic success can be anticipated in the teeth with variations in the number and morphology of canals. To achieve this success, the complex root canal morphology should be thoroughly understood complete evaluation of radiograph is equally important prior to the endodontic treatment. Endodontic exploration using magnification tools such as dental operating microscope (DOM) helps in the identification of an extra canal. Fail to detect the additional root canals, are the major reason for the endodontic failure.[2] Mandibular canines normally have a single root with one canal; but in rare cases there will be extra root or canal.
According to the study conducted by Sikri and Kumar[7] on permanent human mandibular canines They found the canal configurations (Vertucci's). Type I (70%), Type II (4-12%), Type III (4-6%), Type IV (4-10%), Type V (2%), straight canals (53.84-60.71%), curved canals (46-39%), apical foramen centrally located (34.61-57.14%), and apical for a man laterally located (65.38-42.85%).[3]
Two roots may be observed separately radiographically when bifurcation is present either in the cervical or in middle thirds, whereas bifurcation which is present more apically is difficult to diagnose. In the present article, the presence of the two roots was suspected on intraoral periapical as buccal root was present slightly mesially as compared to the lingual root and there was no exact superimposition of both the roots in angled radiograph.[6] Successful endodontic treatment requires knowledge of biology, physiology and root canal anatomy. It also requires proper instruments and the knowledge to use these instruments effectively in teeth with extra roots and canals.Inability to identify and treat these additional root canals may cause treatment failures.[7]
Two mandibular canines were reported in the present case. One tooth has single root, and the other one has two roots. The incidence of two root canals in single & #8209;rooted mandibular canine teeth has been reported to be up to 6.25% and 14% of mandibular canine having Type II canals in mandibular canine. In this article two clinical cases with two roots two canals and one root, two canals were reported in a mandibular canine. The incidence of two canals in mandibular canine was reported more in female than male. Careful interpretation of conventional periapical radiographs taken at more than one angle is necessary to detect variations of teeth morphological. Recently, advanced diagnostic radiographic tools such as cone & #8209; beam computed tomography (CBCT) are very helpful to diagnose morphological variations if conventional radiographic techniques provide lack information and more details are required.[8] Careful examination of preoperative radiographs can aid in locating extra canal or roots. Thus, root canal therapy of these teeth should be carried out by using X-rays from different angulations, efficient explorers and adequate illumination. Necessary precautions have to be taken during root canal therapy of these teeth and hence instrumentation of these canals was carried out using nickel titanium files, due to their flexibility, lesser risks of ledge formation and perforations.[7]
Conclusion
Although the incidence of mandibular canine with two roots and two or three canals is smaller amount but it can occur. An entire knowledge of the tooth and root canal morphology, clinical exploration, detailed radiographic interpretation and advanced radiographic technique will be helpful in detecting root canal aberrations and to achieve success.
Source of Funding
None.
Conflict of Interest
None.
References
- P Bawa, S Gaddalay, A Kale. Mandibular Canin With Two Root Canals. J Med Sci Clin Res 2017. [Google Scholar] [Crossref]
- V A Kumar, A K Gupta, V Sharma, Salil. Endodontic management of mandibular canine withtype two canal configuration: A case report. Int J Appl Dent Sci 2020. [Google Scholar]
- V Arora, V Nikhil, J Gupta. Mandibular Canine with Two Root Canals – An Unusual Case Report. Int J Stomatological Res 2013. [Google Scholar] [Crossref]
- N Borkar, S Bagwe. Root Canal Treatment of Single Rootedmandibular Canine with Two Root Canals: A Report of Two Cases.. J Dent Med Sci 2020. [Google Scholar] [Crossref]
- M Doumani, A Habib, M A Alhenaky, S H Khaled, M S Alotaibi, Alanazi. Anas Alsalhani Root canal treatment of mandibular canine with two root canals: A case report seriesJournal of. J Fam Med Prim Care 2019. [Google Scholar] [Crossref]
- A Malik, P Bansal. Biradicular mandibular canine: A review and report of two cases. Endodontology 2018. [Google Scholar] [Crossref]
- N Shrivastava, V Nikhil, V Arora, M Bhandari. Endodontic management of mandibular canine with two canals. J Int Clin Dent Res Organ 2013. [Google Scholar] [Crossref]
- M A Alenezi, A Yo Al-Hawwas. Permanent mandibular canine with two roots and two root canals: Two case reports. Saudi Endod J 2016. [Google Scholar] [Crossref]