- Visibility 61 Views
- Downloads 1 Downloads
- DOI 10.18231/j.ijce.2024.043
-
CrossMark

Ribbond fiber in root canal rehabilitation: A case report on reinforcement of weakened tooth structures
Introduction
Dentistry is known for its innovations, and we are discussing Ribbond as a promise for the future. Ribbond is a revolutionary dental material engineered from Ultra High Molecular Weight Polyethylene (UHMWPE) fibers, setting a new standard in restorative dentistry.[1] This magical fiber was introduced into dentistry in 1992. Its unique combination of strength, adaptability, biocompatibility, and aesthetic appeal makes it an indispensable tool for dental professionals. Unlike traditional reinforcement materials, Ribbond requires no additional tooth preparation, streamlining the restorative process. They exhibit excellent adaptability to tooth morphology, reducing microleakage and polymerization shrinkage.[2] Moreover, its ability to dynamically adjust interfacial stresses during composite resin photopolymerization ensures long-lasting, durable restorations. [3] This innovative material not only enhances the performance and longevity of dental restorations but also reflects a significant evolution in the approach to dental care, offering a versatile and effective solution for a wide range of clinical applications which include reinforcement of normal composite restoration and orthodontic appliances; fixed partial denture; splinting and so on. They are also being used for endodontic post and core treatment.[4] In addition to its mechanical benefits, Ribbond offers excellent aesthetic outcomes due to its translucent fibers, which allow natural light transmission, blending seamlessly with composite resins. This makes it particularly useful in restoring anterior teeth where aesthetic considerations are paramount. Furthermore, Ribbond’s adaptability allows it to conform to the unique shapes and curvatures of the tooth, ensuring a snug fit and optimal reinforcement of the remaining tooth structure.
Case Report
A 16-year-old male patient presented to the Department of Conservative Dentistry and Endodontics with a fractured upper front tooth (#22) resulting from trauma sustained 5 years ago ([Figure 1]). The patient had undergone initial root canal therapy, but the treatment remained incomplete. Upon clinical examination, an Ellis Class IV fracture was noted on tooth #22. The patient reported no pain or tenderness, and there was no evidence of intraoral swelling or sinus tract. Radiographic evaluation (IOPAR) revealed a wide-open apex with thin remaining dentinal walls, but no signs of periapical radiolucency, indicating the absence of active infection.
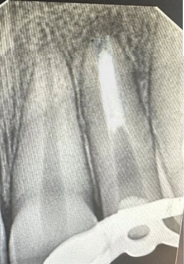
The working length was established ([Figure 2]), and the root canal was disinfected 1 mm short of the apex using a combination of 1% sodium hypochlorite (NaOCl), saline, 2% chlorhexidine (CHX), and 17% EDTA solution. To ensure thorough disinfection and promote healing, intracanal medicament was placed in between the appointments consisting of calcium hydroxide (Ca(OH)₂) or triple antibiotic paste. After ensuring disinfection apexification was performed using mineral trioxide aggregate (MTA), a biocompatible material known for its excellent sealing properties in cases of open apices. Post-operative radiographs confirmed the successful placement of MTA at the apex ([Figure 3], [Figure 4]).
Once apexification was completed, a post and core reconstruction was performed using a polyethylene fiber post-core system -Ribbond ([Figure 5]), which provided support to the thin dentinal walls. This fiber-reinforced composite post is known for its flexibility and strength, making it ideal for cases like this where the remaining tooth structure is fragile. A composite resin was used for the final restoration, providing an aesthetic and durable solution. Immediate post-operative radiographs were taken ([Figure 6]), and the patient was followed up for one year, showing satisfactory clinical and radiographic outcomes ([Figure 7]).






Discussion
The preparation of cavities substantially impacts the compressive strength and stress distribution within the tooth. [5] Therefore, clinical approaches that can improve the fracture resistance of compromised teeth and improve the clinical longevity of dental restorations are critical to improving the quality of dental service.[6]
Ribbond: A spectrum of 215 fibers,was invented by Dr.David N Rudo. It has been demonstrated that ribbond fibers can increase the flexural strength and fracture toughness of composite resin restorations.[7] They are withstanding impact strength five times greater than iron and are made from the same fibers used to make bulletproof vests. The fiber design based on a dense network of locked nodal intersections can act as a crack stopping mechanism by changing the direction that ultimately dissipates strain.[8]
Ribbond boosts composite resin strength and microtensile bond in high C-factor cavities. The "gas plasma" treatment reduces fiber tension ensuring a strong chemical bond with composite materials. Ribbond’s translucent fibers take on the color characteristics of the composite and allow for the natural transmission of light through restoration and crowns.
Fracture of anterior teeth is the most common in permanent dentition. Root canal therapy (RCT) is effectively done after apexification but compromised dentinal walls particularly in cervical area, makes these teeth vulnerable to fracture.[9] The fracture resistance of endodontically treated teeth mainly depends on the remaining dentine thickness around post and core systems. Flared root canals are more vulnerable to fracture because the remaining walls are thin, and therefore the restoration of those teeth requires techniques which will not compromise the integrity of the remaining radicular tooth structure. Fibre reinforced composite root canal posts with an elastic modulus close to that of dentin were introduced in the 1990’s. They were found to reduce the incidence of root fracture, and, in the case of endodontic retreatment, they could be removed from the root canal with ease [10] and predictability without compromising core retention.[11]
Ribbond fibers have proven effective in reinforcing weakened root structures. Research indicates that in flared root canal the C-factors in dowel spaces can reach as high as 200, may contribute to marginal leakage when utilizing prefabricated fiber or zirconia dowel systems. Ribbond acts as a "shock-absorber," preventing strain energy build-up and stress concentration, thereby averting cracks and potential catastrophic failures in the dental-restorative complex.
The mean survival was 90.2% after the follow-up period 97 months in teeth restored with fiber-reinforced post- &core buildups. [7] The utilization of UHMWPE fiber reinforcement systems presents a promising avenue for addressing the challenges associated with root canal rehabilitation, particularly in cases where root canals are characterized by thin and flared dimensions. These fibers are advantageous because they can bond to dentine, which helps in reinforcing the remaining tooth structure without the need for further enlargement of the root canal. [8] They provide adaptability to the root canal walls without the need for additional canal enlargement after endodontic treatment, also they reinforce weakened root canal system.
In recent years, the application of fiber-reinforced systems like Ribbond in restorative dentistry has gained considerable attention due to their ability to enhance the durability and functionality of compromised teeth. One of the key advantages of Ribbond fibers is their ability to minimize the invasive nature of traditional post systems. Conventional post-and-core systems often require significant enlargement of the root canal, which can lead to further weakening of the tooth structure. By contrast, Ribbond fibers offer a conservative approach that focuses on maintaining as much of the natural tooth structure as possible, an essential factor in the long-term survival of endodontically treated teeth. The fibers can be shaped and molded to adapt to even the most irregular canal shapes, which makes them particularly effective in cases where standard dowel systems would fall short. [12] For root canals with thin walls, materials such as glass or quartz fiber posts, MTA, Biodentine, and self-adhesive resin cements are ideal for reinforcing the structure while creating a monoblock effect. Fiber posts distribute stresses evenly, while MTA and Biodentine provide bioactivity and strong adhesion with dentin, enhancing canal wall support. Combined with bioceramic sealers or calcium silicate-based sealers, these materials bond well, minimizing microleakage and reducing fracture risk in compromised roots. [13]
Conclusion
In conclusion, successful post-endodontic restoration is crucial for the long-term survival of root canal-treated teeth, especially in cases with compromised tooth structure. The use of innovative materials like "Ribbond" offers not only a reliable solution but also represents the future of dental reinforcement. Its strength, flexibility, and biocompatibility make it an ideal choice for reinforcing weakened teeth, ensuring both functionality and durability while preserving aesthetics. By integrating advanced materials like Ribbond, modern dentistry continues to evolve, providing patients with superior outcomes and long-lasting restorations. Therefore “Ribbond” isn’t just a solution; it's the future of dentistry woven into every fiber.
Conflict of Interest
None.
Source of Funding
None.
References
- JM Bae, KN Kim, M Hattori, K Hasegawa, M Yoshinari, E Kawada. Fatigue strengths of particulate filler composites reinforced with fibers. Dent Mater J 2004. [Google Scholar]
- MK Hasija, B Meena, D Wadhwa, V Aggarwal. Effect of adding ribbond fibres on marginal adaptation in class II composite restorations in teeth with affected dentine. J Oral Biol Craniofac Res 2020. [Google Scholar]
- V Chaudhary, B Shrivastava, H P Bhatia, A Aggarwal, AK Singh, N Gupta. Multifunctional Ribbond--a versatile tool. J Clin Pediatr Dent 2012. [Google Scholar]
- N Tuloglu, S Bayrak, E S Tunc. Different clinical applications of bondable reinforcement ribbond in pediatric dentistry. Eur J Dent 2009. [Google Scholar]
- I Kantardzić, D Vasiljević, L Blazić, O Luzanin. Influence of cavity design preparation on stress values in maxillary premolar: a finite element analysis. Croat Med J 2012. [Google Scholar]
- RT AlJarboua, RA Alshihry, HO Alkhaldi, FHA Marar, MA Aljaffary, ML Almana. Effect of Fiber-Reinforced Composite Placement Site on Fracture Resistance of Premolar Teeth: An in vitro Study. Clin Cosmet Investig Dent 2024. [Google Scholar] [Crossref]
- S Akman, M Akman, G Eskitascioglu, S Belli. Influence of several fiber-reinforced composite restoration techniques on cusp movement and fracture strength of molar teeth. Int Endod J 2011. [Google Scholar]
- T Sfeikos, D Dionysopoulos, P Kouros, O Naka, K Tolidis. Effect of a fiber-reinforcing technique for direct composite restorations of structurally compromised teeth on marginal microleakage. J Esthet Restor Dent 2022. [Google Scholar]
- S Singh, R Nagpal, P Singh, UP Singh, N Manuja. Esthetic and Functional Rehabilitation of Maxillary Anterior Tooth by Polyethylene Fibre Post. Austin J Clin Case Rep 2016. [Google Scholar]
- B Akkayan, T Gülmez. Resistance to fracture of endodontically tretaed teeth restored with different post systems. J Prosthet Dent 2002. [Google Scholar]
- M L Pitel, N L Hicks. Evolving technology in endodontic posts. Compend Contin Educ Dent 2003. [Google Scholar]
- J Bijelic-Donova, T Myyryläinen, V Karsila, PK Vallittu, J Tanner. Direct Short-Fiber Reinforced Composite Resin Restorations and Glass-Ceramic Endocrowns in Endodontically Treated Molars: A 4 -Year Clinical Study. Eur J Prosthodont Restor Dent 2022. [Google Scholar]
- S Akman, M Akman, G Eskitascioglu, S Belli. Influence of several fibre-reinforced composite restoration techniques on cusp movement and fracture strength of molar teeth. Int Endod J 2011. [Google Scholar]