Introduction
The main goal of endodontic treatment is to restore or preserve the health of the periapical tissues by thoroughly cleaning and filling the root canal system.1 To achieve this, clinicians must have a solid grasp of root and canal morphology, including any variations. A common cause of endodontic failure is missed canals, making it essential to have a comprehensive understanding of root canal anatomy to accurately identify and diagnose variations before beginning treatment. 2
Recent studies conducted on the Indian population have revealed various anatomical variations in maxillary second molars through CBCT analysis. These studies indicate that the presence of a single root and canal in maxillary second molars is rare, with an incidence rate ranging from 0% to 3.1%.3, 4 This case series discusses two cases involving the diagnosis and treatment of symptomatic irreversible pulpitis (SIP) in maxillary second molars with a single root and canal.
Case Series
Case 1
An 18-year-old male patient presented with a chief complaint of pain in the upper right back tooth region, persisting for the past week. The pain developed gradually was localized, and worsened with chewing and cold food intake, though it was temporarily alleviated by medication. In the last two days, the patient also experienced nocturnal pain. Clinical examination revealed deep caries in the maxillary right second molar. Pulp sensibility tests, including cold and electric pulp tests (EPT), indicated a delayed and lingering response. Radiographic evaluation showed radiolucency extending to the pulp, with no evidence of periapical pathology. Based on these findings, a diagnosis of symptomatic irreversible pulpitis (SIP) was made, and endodontic treatment was planned. The preoperative radiograph suggested the presence of a single root with a single canal (Figure 1a). To confirm the canal anatomy and rule out additional canals, cone-beam computed tomography (CBCT) was performed. CBCT images confirmed the presence of a single large central canal within a single conical root (Figure 1b,c).
During the initial visit, local anesthesia (Lignox 2%, Kilitch Drugs India Ltd., Navi Mumbai, India) was administered, and the access cavity was prepared under rubber dam isolation. After removing the caries, a single large oval canal was exposed at the center of the tooth (Figure 1d). The working length was established using an electronic root canal length-measuring device (J Morita USA, Inc.) and confirmed radiographically (Figure 1e). Canal preparation was carried out using ISO hand K-files (Mani, Germany) up to size #80.02 (Figure 1f). Irrigation with 2 ml of 3% sodium hypochlorite (Parcan, Septodont Healthcare India Pvt. Ltd, Maharashtra, India) was performed after each instrument, followed by a final rinse with 17% ethylenediaminetetraacetic acid (DeSmear, Anabond, Chennai, India) and saline. Sonic activation of the irrigant was done using an Endo Activator (Dentsply Sirona Inc, USA) placed 2 mm short of the apex. After drying the canal with sterile paper points, it was obturated using the Thermoplasticized obturation technique with gutta-percha (Calamus, Dentsply Sirona Inc, USA) and AH Plus sealer (Dentsply, Maillefer, USA). The access cavity was then restored with flowable composite (Filtek Z350 XT, 3M ESPE, St. Paul, MN, USA), and a post-obturation radiograph was taken.
During the second visit, the tooth was prepared for a lithium-disilicate endocrown. Putty and light-body polyvinyl siloxane impressions (GC Flexceed, GC India Dental Pvt., India) were made. In the final visit, the intaglio surface of the endocrown was etched with 9% hydrofluoric acid (Ultradent® Porcelain Etch, Ultradent Products GmbH, Germany), followed by the application of a silane coupling agent (Silane, Ultradent Products GmbH, Germany). The tooth surface was etched with 37% phosphoric acid (D-tech XT Etch, India) for 15 seconds, rinsed, and treated with a bonding agent (G-Premio Bond, GC Corporation, Tokyo, Japan). The endocrown was cemented using dual-cure resin cement (RelyX U200, 3M ESPE, St. Paul, MN, USA), and a radiograph was taken to confirm the fit (Figure 1g).
Case 2
A 38-year-old female patient presented with a chief complaint of pain in the upper right back tooth region for the past three weeks. The patient exhibited signs and symptoms similar to those in Case 1. Clinical examination revealed deep caries in the maxillary second molar, and pulp sensibility tests indicated a delayed response. Radiographic evaluation showed radiolucency extending to the pulp with no evidence of periapical pathology (Figure 2a). Based on these findings, a diagnosis of symptomatic irreversible pulpitis (SIP) was made, and endodontic treatment was planned. Cone-beam computed tomography (CBCT) was performed to confirm the canal anatomy (Figure 2b,c).
Figure 1
CASE 1 a: Pre-op Radiograph; b: CBCT axial view; c: CBCT coronal view; d: Access Opening; e: Working Length Radiograph; f: Master cone Radiograph, and g: Post-op radiograph
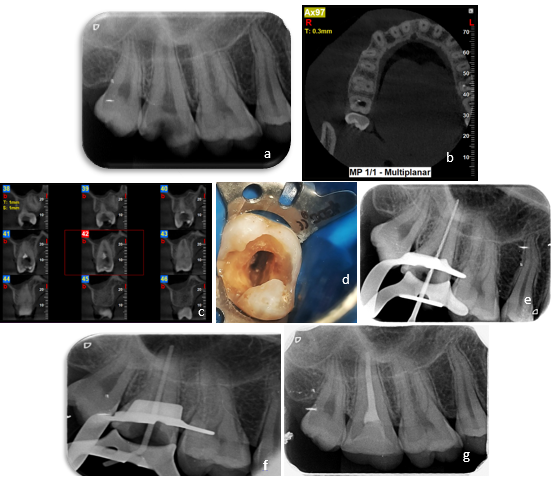
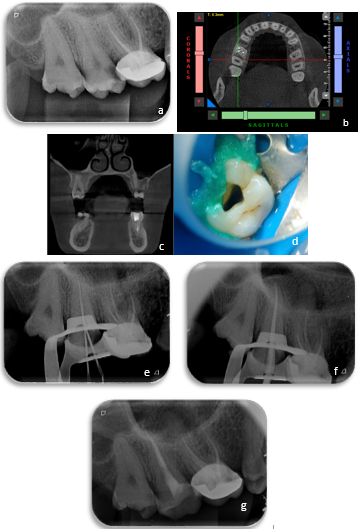
Figure 2
CASE 2 a: Pre-op Radiograph; b: CBCT axial view; c: CBCT sagittal view; d: Access Opening; e: Working Length Radiograph; f: Master cone Radiograph, and g: Post-op radiograph
After administering local anesthesia and isolating the tooth with a rubber dam, an access cavity was prepared, revealing a wide single canal. Following the determination of the working length, biomechanical preparation and obturation were performed, following the same protocol as in Case 1 (Figure 2d,e,f). The tooth was then prepared for a lithium-disilicate inlay, and impressions were taken. During the next visit, the inlay was cemented using dual-cure resin cement, following the same procedure as in Case 1. A final radiograph was taken to verify the fit (Figure 2g).
Discussion
Understanding root canal anatomy thoroughly is crucial because neglecting any unexplored canals can result in treatment failure. The typical morphology of maxillary molars often involves three roots and three to four canals. Advancements in imaging techniques have revealed anatomical variations in maxillary second molars frequently, for example exhibiting a Vertucci’s type I canal configuration, similar to the cases discussed in this series.
In single-rooted maxillary molars, the roots can be categorized as pyramidal, fused, or conical based on their morphology. In the pyramidal type, the roots are completely fused, resulting in a single enlarged root canal.5 The prevalence of single-rooted maxillary molars is higher in the Asian population. A 2012 study found that the incidence of single-rooted maxillary molars in Koreans was 0.25%. 6 Similarly, a 2011 study using CBCT on the Chinese population reported a 10% incidence of single roots in maxillary second molars. In these cases, the root canal system may feature a single wide canal, two canals that may or may not merge, or a C-shaped canal. 7
The search for a missing canal can often result in iatrogenic complications, such as perforation or excessive removal of tooth structure. These issues can be prevented if the clinician has a solid understanding of potential variations in the root canal system. A thorough preoperative assessment, including multiple angled radiographs and the use of CBCT in cases of uncertainty about the canal anatomy, is essential to avoid such errors. 8
Traditional intraoral periapical radiographs play a vital role in endodontics for evaluating root morphology and canal configuration. In our cases, suspicions regarding the canal configuration of the maxillary second molar were initially raised through an intraoral periapical radiograph. While conventional radiography remains important, it does have limitations. New diagnostic tools like CBCT and Micro CT have addressed these drawbacks by generating three-dimensional images. Hence, CBCT was used to confirm the canal configuration and the absence of additional canals. CBCT offers a non-invasive method for identifying anatomical variations in root canals, facilitating comprehensive debridement of the entire root canal system, and enhancing the predictability of endodontic procedures. 9, 10, 11
Posterior indirect adhesive restorations are now widely used in clinical practice. These restorations allow for the conservation of tooth structure while leveraging the mechanical advantages of modern adhesive technology, which helps reinforce weakened teeth. 12 Endocrowns, in particular, are conservative restorations designed for endodontically treated teeth with substantial coronal tooth structure loss. These monoblock restorations are supported by the pulp chamber and bonded to the remaining coronal tooth structure for retention. A systematic review and meta-analysis conducted by Al-Dabbagh et al., in 2020 compared the 5 years survival rate of endocrowns and conventional crowns and concluded that endocrowns showed a 91.4% survival rate and 77% success rate which was not a statistically significant difference from conventional crowns. 13 Similarly, Spitznagel et al., in 2023 analyzed the performance and failure load of partial-coverage restorations with single crowns and concluded that minimally invasive LDS partial-coverage restorations showed superior results compared to single crowns.
Conclusion
The presence of maxillary second molars with a single root and canal is uncommon, early diagnosis is crucial for successful endodontic treatment. CBCT should be employed in such cases when conventional radiographs fail to conclusively identify canal anatomy, preventing unnecessary dentin removal in search of additional canals. This case series demonstrates the effective endodontic management of such cases, followed by minimally invasive post-endodontic restorations.